Definition
Carpal tunnel syndrome (CTS) is the most common peripheral nerve entrapment word wide. The general trend for this condition is progressive worsening, although spontaneous regression of symptoms is possible. Patients can be diagnosed quickly and respond well to treatment but the best means of integrating clinical, functional, and anatomical information for selecting treatment choices has not yet been identified.[1][2]
Clinically Relevant Anatomy

Walls
The carpal tunnel (CT) is formed by non extendable osteofibrous wall surrounding its content. The wall of the tunnel tunnel consists of carpal bones, joint capsule, carpal ligamets, flexor carpi radialis tendon and the flexor retinaculum. Carpal bones form an arch like base for the tunnel. Flexor retinaculum spanning from the pisiform bone and the hamulus of the hamate bone to the scaphoid and the trapezium complete and close the tunnel. [3] [4]
The eight carpal bones are oriented in two rows between the ulna and radius and the metacarpal bones. These form an articulated connection between the forearm and the hand.
Content
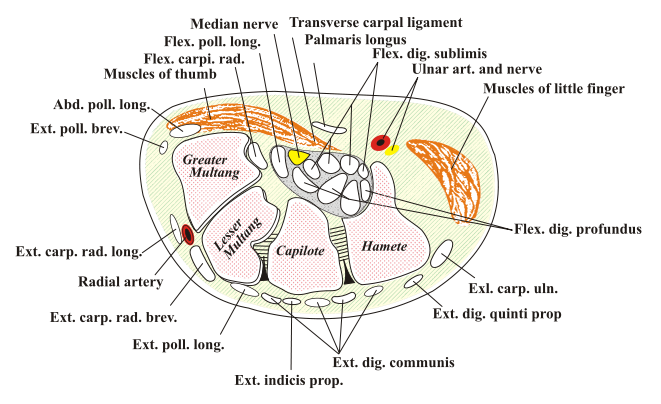
CT allows passage of multiple structures between hand and proximal segments of body (Picture 2). Tendons of flexor digitorum profundus, flexor digitorum superficialis and flexor pollicis longus muscles and the median nerve form the content of carpal tunnel. The median nerve passes from the forearm to the palmar aspect of the hand, Its sensory axons convey sensory stimulation for median nerve distribution consisting of palmar aspect of thumb and fingers, except for the fifth digit and ulnar half of fourth digit. Motor axons of median nerve supply the muscles of thenar eminence. [5]
Etiology and epidemiology[2]
The estimated prevalence of CTS is 4-5% of the population.There are two peak age frequencies: the first and biggest peak is between 45 and 59 years of which 75% is female. The second age peak is between 75 and 84 years, of which 64% is femal.Most cases of CTS are idiopathic, A portion of incidences of CTS are caused by pathological changes in structures passing through the carpal tunnel or the tissues forming it’s walls. Finally, considerable proportion of CTS cases are linked to pathological demands on wrist motion.
Idiopatic carpal tunnel syndrome
- Idiopathic CTS occurs more frequently in females (65–80%) and between the ages of 40 and 60 years; 50–60% of the cases are bilateral.[6]
- The bilateral characteristic increases in frequency with the duration of symptoms.[7]
- Idiopathic CTS is correlated with hypertrophy of the synovial membrane of the flexor tendons caused by degeneration of the connective tissue, with vascular sclerosis, edema and collagen fragmentation.[8] The histological changes were thought to be suggestive of dynamic factors as repetitive strain.
- Predisposing factors based on meta-analyses conducted in 2002[9] and 2008,[10] include:
- sex
- age
- genetic and anthropometric factors (size of the carpal tunnel) were of most importance followed by other correctable predisposing factors of clinical importance as:
- besity
- smoking
- excessive alcohol consumption
- repetitive manual activities and exposure to vibrations and cold temperatures were the least important and of little clinical relevance
Secondary carpal tunnel syndrome
Abnormalities of the walls of CT
- Any condition that modifies the walls of the carpal tunnel may cause compression of the median nerve.[11]
- Abnormalities of the shape or position of the carpal bones: dislocation or subluxation of the carpus[11][12]
- Abnormalities of the shape of the distal extremity of the radius: fractures (translation of more than 35%)[13] or skewed consolidation of the distal radius; osteosynthesis material on the anterior face of the radius;[14]
- Joint abnormalities: wrist arthrosis,[15] inflammatory arthritis[16] (due to synovial hypertrophy, bone deformation an/or carpal shortening), infectious arthritis,[17] rhizarthrosis[18] or villonodular synovitis[19]
- Acromegaly.[20]
Abnormalities of the content of CT
- Tenosynovial hypertrophy;
- Inflammatory tenosynovitis: inflammatory rheumatism[16] lupus and infection
- Metabolic tenosynovitis: diabetes mellitus[21] (abnormality of collagen turnover), primary or secondary amyloidosis (chronic hemodialysis with deposition of beta-2-microglobulin),[22] gout[23] and chondrocalcinosis;[24]
- Abnormalities of fluid distribution: pregnancy[25][26] in 0.34% to 25% of the cases, especially in the third trimester, with frequent signs of deficit in 37–85% of the cases; hypothyroidism[27] and chronic kidney failure (arteriovenous fistula).[22]
- Abnormal or supernumerary muscle: deep palmar muscle[28] intratunnel position of the muscle body of the superficial flexor[29] or proximal extension of the muscle body of the lumbrical muscles[30]
- Persistent arterial hypertrophy of the median nerve
- Intratunnel tumor: lipoma, synovial cyst, synovial sarcoma or neural tumor (schwannoma, neurofibroma or lipofibroma);
- Hematoma: hemophilia[31] anticoagulant accident[32] or trauma[33]
- Obesity[34]
Dynamic carpal tunnel syndrome
The pressure inside the carpal tunnel increases during wrist extension and flexion[35] Repetitive extension and flexion movements of the wrist, along with flexion of the fingers and supination of the forearm, have been implicated in this increase[36] Incursions of muscle bodies from the superficial and deep flexors of the fingers, when the wrist and fingers are extended, have been found in 50% of the cases This particular movement can be seen in occupational pathological conditions[37]
Computer work and CTS
No increase in the prevalence of CTS in cases of working on computers for more than 15 h per week has been observed. A tendency toward increased prevalence has been demonstrated in cases of working on computers for more than 20 h per week[38]
Exposure to vibration
Exposure to vibration is one of the lesser predisposing factors.[27][10] The ultrastructural consequences comprise microcirculatory compression problems and intraneural edema following injury of the myelin and axons.
Occupational factors
Occupational biomechanical factors play a substantial role in the causation of CTS. Data from current primary studies on dose-response suggest that the risk of CTS increases with the [39]
Acute CTS
Etiologies:
- Trauma: displacement due to fracturing of the distal radius or dislocation of the wrist;
- Infection;
- Hemorrhage due to overdose of anticoagulant or in cases of hemophilia;
- High-pressure injection;
- Acute thrombosis of the artery of the median nerve;
- Burns.
Clinical presentation

CTS onset is generally gradual with tingling or numbness in median nerve distribution of affected hand. Fig.3. [41] [42] [43]
Patients may notice aggravation of symptoms with static gripping of objects as phone or steering wheel but also at night or early in the morning. [42] [43] Many patients will report improvement of symptoms following shaking or flicking of their hand.
As the disorder progresses, the feeling of tingling or numbness may become constant and patients may complain of burning pain. [42]
The final symptoms are weakness and atrophy of muscles thenar eminence.
These combined effects of sensory deprivation and weakness may result in complaint of clumsiness and loss of grip and pinch strength or dropping things, [42]
Differential diagnosis

Process of differential diagnosis should give consideration to all conditions which could potentially cause a dysfunction of median nerve, or its contributories in brachial plexus, C 5 to 8 nerve roots and central nervous system. For example: an injury of nn. digitales in the palm, radiculopathy will overlap with CTS in location of paraesthesia of hand as demonstrated in Fig. 3 and 4.
Other conditions to be aware of when diagnosing CTS include:
Diagnostic procedures
Electroneuromyography (ENMG) examination[41] is used to examine the sensory and motor nerve conductance of the median nerve. It also highlights the elective weakening in passing through the carpal tunnel. It is considered abnormal when there is a diminished sensory conduction velocity between the wrist, the palm of the hand and the fingers. This test may be used to diagnose the condition and rule out other pathologies. [2]
Electromyogram (EMG) of the muscles innervated by the median nerve measures electrical dischargers produced in the muscles. This test can determine if there is any muscle damage and can rule out other conditions. [46] [47]
Ultrasonography can identify space-occupying lesion in and around the median nerve. The test can confirm abnormalities that can diagnose CTS and help guide steroid injections into the carpal tunnel. [41] [48]
X-ray is recommended to exclude other causes of wrist pain like arthritis or bony pathology. [2]
Outcome measures
There are several questionnaires available to determine the outcome measures for CTS. The four questionnaires below are all supported by studies with level of evidence 2A or 2B. Only the study of Levine et al. [49], describing the BCTQ, has level of evidence 4. This questionnaire is, however supported by other, higher level studies as well.
1. Boston Carpal Tunnel Questionnaire (The BCTQ or the Levine Scale, originally developed by Levine et al. (1993) [49], is the most commonly used outcome measure in the assessment of CTS patients. It can be self-, interview- or telephone-administered. The questionnaire comprises of two scales: the Symptom Severity Scale (SSS) and the Functional Status Scale (FSS). [50] [51]
The SSS consist of 11 questions, scored on a five-point rating scale, for the evaluation of pain, test-retest reliability of paraesthesia, numbness, weakness, nocturnal symptoms and overall function status. [50] [51]
The FSS rates 8 functional activities on difficulty level, also scored on a five-point rating scale. The overall score for both scales is calculated as the mean of the items. [51]
The reliability, validity and responsiveness of the BCTQ has been found to be very good by several studies, such as the report of the University of Oxford16 and the studies of Sambandam et al. [51], Bakhsh et al. [52] and Greenslade et al. [53].
2. Disability of Hand and Shoulder (DASH) Questionnaire
The DASH-questionnaire is a self-, interview- or telephone-administered region-specific outcome instrument developed as a measure of self-rated upper-extremity disability and symptoms. The DASH is a 30-item scale, each scored on a 5-point Likert scale and overall scored on a scale from 0 (no disability) to 100 (maximum disability). It consists of two dimensions: Physical Functioning and Symptoms. The DASH is not specific for CTS, but can detect and differentiate small and large changes in disability over time after surgery in patients with several upper extremity musculoskeletal disorders. [50]
The DASH questionnaire is also found to be a valid and reliable test with good responsiveness. [50] [51] [53] [54] Bakhsh et al. [52] however found the DASH questionnaire to be less responsive than the BCTQ.
3. Michigan Hand Outcomes Questionnaire (MHQ)
The MHQ is a self-, interview- or telephone-administered questionnaire used to assess the outcome for various hand disorders. [50] It consists of 37 items, grouped into 6 domains: overall hand function, activity of daily living, pain, work performance, aesthetics and patient satisfaction with hand function. All questions are scored from 1 to 5, with high scores denoting better performance, except for the pain scale, in which a higher score means more pain. The score of each scale is converted to a score from 0 to 100. [50] [51]
The MHQ is found to be a valid and reliable measurement with good responsiveness. [50] [51]
A short 12 item version was also validated for CTS and several other common hand conditions to reduce the burden and promote its use in clinical setting.[55]
4. Patient Evaluation Measures (PEM)
The PEM is a self-, interview- or telephone-administered questionnaire to measure physical health. It consists of 3 components (patient’s opinion on delivery of care, hand health profile, overall assessment) and a total of 18 items scored on a 7-point scale. Low scores indicate positive outcomes.16 17 Hobby et al.20 found this instrument to be valid and reliable and to have good responsiveness. [50] [51]
Examination
Clinical prediction rules (CPR), specifically for the Carpal Tunnel Syndrome, are a reliable examination method. It consists of five tests. Wainner et al. [56] found that the CPR is more useful for diagnosis of CTS than any single test item. Using CPR results is posttest probability changes up to 56%.
Other than the CPR, there are several provocative tests and the thenar atrophy observation that can be used in the clinical examination of a CTS patient. In Table 2 [58] you find the sensitivity and specificity rates of all the tests explained below.
| Sensitivity (%) | Specificity (%) | Positive Prediction Value (%) | Negative Prediction Value (%) | Accuracy (%) | |
| Scratch Collapse Test | 34 | 61 | 71 | 25 | 41 |
| [58] [59] [60]
Provocative tests: 1. [60], the patient holds his forearm vertically and lets his wrist drop down in 90° flexion [61]. The arm can also be held horizontally in front of the patient with the wrist hanging down. [62] Another common way of executing the test is to hold both wrists against each other in 90° flexion with elbows also flexed and fingers pointing in the patient’s direction. [63] [64] 3. Hand elevation test ([61] The test is positive when the patient experiences typical CTS symptoms, such as a numb or tingling feeling in the fingers or pain or stiffness in the fingers, palm or wrist. Some patients also experience soreness in the shoulder. [65] This test is only considered meaningful if the results can be duplicated by other, more specific CTS tests. [65] 4. Scratch Collapse Test (CTS-6 Lax/Sringent) Video of the Scratch Collapse Test: 5. Durkan’s Carpal Compression Test Medical ManagementNon-surgical treatment comprises oral steroids [67] [68], corticosteroid injections [68], NSAID [67][68], diuretics [67][69], vitamin B6 [67] and splinting/hand brace [67][68][69]. Huistede et al [70] concluded that surgical treatment seems to be more effective than splinting and anti-inflammatory drugs plus hand therapy in the midterm and long term to treat CTS [42][68]. However, there is no unequivocal evidence that suggestsone surgical treatment is more effective than the other[42]. The two main manners to decompress the median nerve by surgery are the [71] says that with both techniques (OCTR and ECTR) the structural complications for nerves, blood vessels or tendons are low. According to Chen et al [72] there are no obvious statistical differences in relief of symptoms (pain en paraesthesia), recovery of grip strength a reoperation rate. Though, two articles with moderate to strong level of evidence declares the ECTR causes a faster return to work [72][73] and a better recovery of pinch strength. Physical Therapy managementPatients with mild to moderate symptoms do not need to be immediately operated but can be effectively treated in a primary care environment [74][75] Physical therapy typically consists of modifications of activities and the work place (ergonomic modifications) [74][75], patient education, carpal bone and [76],, ultrasound [67][68][76] and electromagnetic field therapy [67][68] and splinting.[77] It’s important to mention that, in general, the evidence of the effectiveness of the exercise and mobilization interventions is limited and very low in quality. The physical therapist should always inform the patient about the limited evidence of effectiveness and safety as well as availability of surgical option without the pre-requite conservative therapy where appropriate. [76]. The effectiveness of ultrasound varies between the studies and most of the time the evidence is low. According to Page et al [78] there’s poor and limited evidence about the effect of therapeutic ultrasound. There is insufficient evidence that therapeutic ultrasound has a greater benefit than other non-surgical treatments, such as splinting, exercises or oral drugs. It is important to pay attention to the cause of the CTS. Physical therapists should give advice in task modification, like taking fufficient rest and variation of movements. Burke et al [75] declare that often simple obvious alterations to the working practice can be beneficial in controlling milder symptoms of CTS. Peter et al [79] declare that evidence about post-operative rehabilitation is also limited. Their reviewed interventions handle physical applications, differences between kinds of immobilisation and multimodal hand therapy. None of them seems to have a prevailing benefit. Clinical Bottom LinePatients may benefit form physiotherapy based treatment with goals of CTS symptom reduction and functional gains, provided that:
Treatment should be discontinued when shown to be ineffective and appropriate, evidence based discharge recommendations should be made. CTS symptoms typically escalate over a longer term despite conservative treatment. Surgical interventions for appropriate patients have been shown to be safe and more effective than any conservative intervention, Clinicians should be aware that constant tingling or numbness is associated with significant compression of median nerve. Prolonged duration of such symptoms may lead to irreversible changes in its internal structure, affecting effectiveness of surgery and leaving individuals with chronic symptoms and muscle atrophy of thenar eminence. Patients should be followed by their general practitioners to discuss surgical treatment options when necessary and desired. References
×
Ola!Como podemos ajudar? |
